
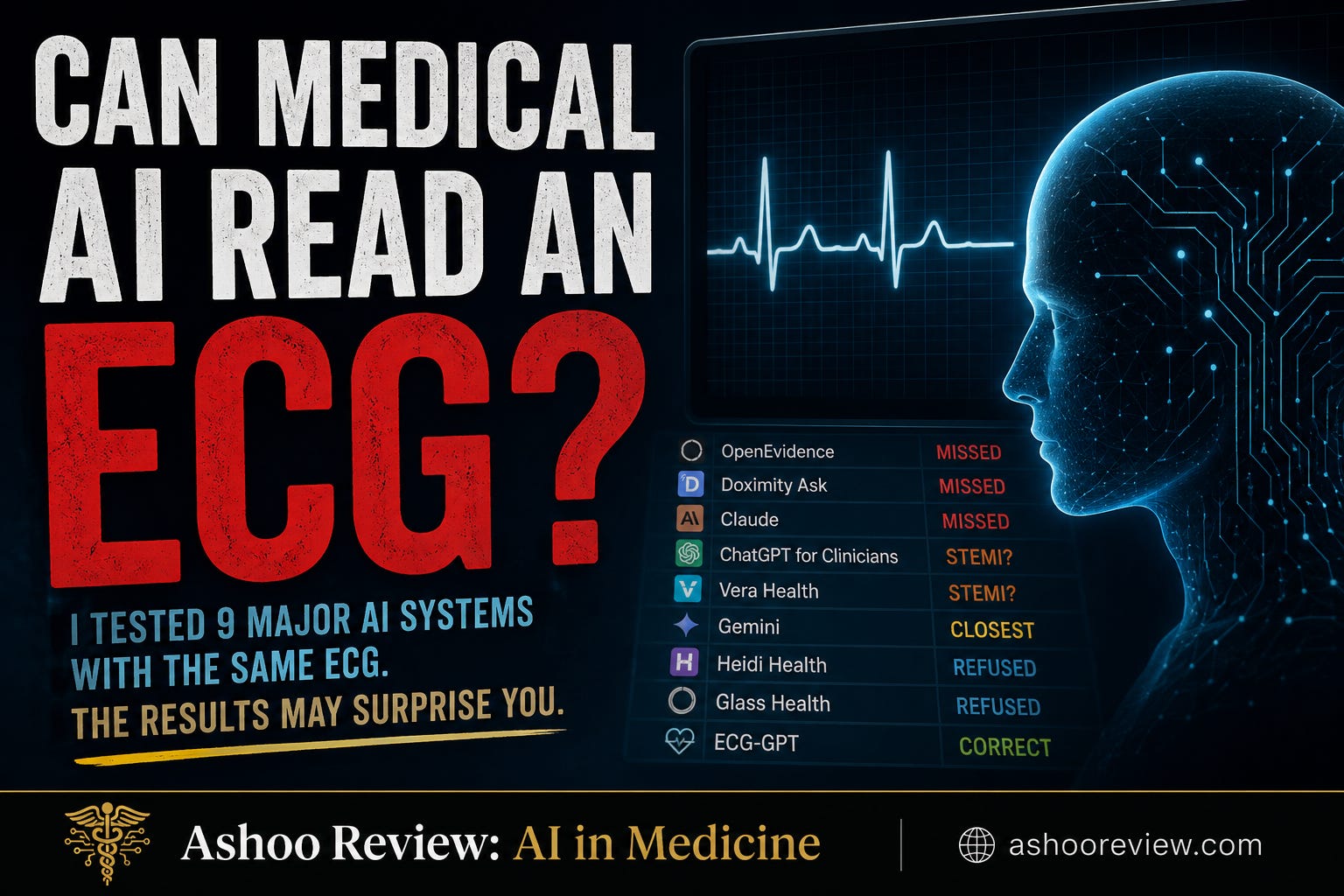
Can Medical AI Read an ECG?

Last week, I published the results of a challenging but routine case posed to 6 AI models. Today, I’m sharing the results of a similar task: reading an ECG. Before you come to the defense of your favorite model, keep one thing in mind: many of these systems are being placed into the hands of clinicians without clear instructions about what they can do, what they can't do, and where they haven't been tested. That's ultimately my biggest concern.
As always, if you enjoy reading the content, consider subscribing and telling a friend. Now let’s get into the details…
Sam
If you’ve been a reader for a while, you know I’ve written about why medical AI companies may shy away from advertising that their models can read ECGs. In my earlier post on FDA regulation and medical AI, I discussed how interpreting signals from medical devices can place a company in a very different regulatory category. That’s one reason you don’t see many AI companies prominently advertising ECG interpretation as a feature, even when their systems can analyze uploaded images.
Yet nearly every major medical AI platform allows file uploads. Upload a PDF, a screenshot, or a clinical image. Ask a question. Get an answer.
For the upload feature, an ECG is simply an image file. This made me wonder: if these systems accept ECG images, can they interpret them?
Before We Begin
Before getting into the results, I should make one thing clear. A model doesn’t have to interpret an ECG to pass this test. In fact, one of the more interesting findings from this experiment is that refusing to interpret may be the safest answer.
If a system says it can’t interpret ECGs, or that ECG interpretation falls outside its capabilities, I don’t consider that a failure. ECG interpretation is a diagnostic activity. There are perfectly reasonable technical, legal, regulatory, and safety reasons for a company to draw that boundary. A model that understands its limitations is demonstrating something important.
The Test ECG
The ECG I chose wasn’t particularly exotic and was not designed to trick the reader.
The reference interpretation was:
Second-degree AV block with 2:1 conduction
Ventricular rate: 36 bpm
Left bundle branch block
QTc: 463 ms
Additional measurements included:
PP interval: 21 small boxes (atrial rate ~71 bpm)
RR interval: 42 small boxes (ventricular rate ~36 bpm)
QT interval: 15 small boxes (600 ms)
Normal axis (~40°)
No Sgarbossa or modified Sgarbossa criteria
What makes the tracing interesting is that the diagnosis isn’t a morphology problem; it’s a counting problem.
The atrial rate is approximately 71 beats per minute. The ventricular rate is approximately 36 beats per minute. Every other atrial impulse fails to conduct. To understand what’s happening, you have to count the P waves, count the QRS complexes, and determine their relationship to one another.
That sounds straightforward. As it turned out, it was surprisingly difficult for the AI systems.
The Refusers
Heidi Health
Heidi declined to interpret the tracing, explaining that ECG interpretation falls outside its scope. No diagnosis, hallucinations, or invented arrhythmias.
Glass Health
Glass Health took a different route and explained that it could only extract OCR text from the image rather than reliably analyze the tracing itself. Again, there was no diagnosis or inappropriate recommendations.
At first glance, these responses may seem disappointing. By the end of the experiment, they looked increasingly sensible.
The Misses
OpenEvidence
OpenEvidence delivered the most surprising result by misclassifying the ECG as atrial fibrillation with a controlled ventricular response of 60 to 80 beats per minute and raising concern for anterior STEMI.
The actual tracing contained a ventricular rate of 36 and left bundle branch block. This wasn’t simply a missed diagnosis. The system effectively described a different ECG from the one it had been shown.
Doximity Ask
Doximity identified a sinus rhythm at 70 beats per minute, which immediately caught my attention because the atrial rate was approximately 71.
It appears the model successfully identified sinus node activity, but never realized that only every other impulse was conducting. The diagnosis drifted toward left anterior fascicular block and possible old posterior infarction, while the actual conduction abnormality remained unrecognized.
Claude
Claude followed a similar path. It identified a sinus rhythm and a normal axis but focused on poor R-wave progression as the dominant abnormality.
Much like the others, the final reading described a different ECG from the one presented.
The STEMI Hunters
ChatGPT for Clinicians
ChatGPT for Clinicians was the first model to correctly identify the left bundle branch block. That deserves credit because several of the other systems missed it entirely.
Once it recognized the LBBB, the model shifted to possible acute coronary occlusion and discussed the modified Sgarbossa criteria, though the reference interpretation had neither finding.
In other words, it recognized the conduction abnormality but then overcalled the ischemic significance.
Vera Health
Vera Health behaved similarly. It generated a differential diagnosis centered on LAD occlusion, De Winter pattern, Takotsubo syndrome, and anterior STEMI.
Reading the interpretation, I had the sense that the model was highly attuned to ischemic pattern recognition while largely overlooking the conduction problem.
The Closest Answer
Google Gemini
Gemini was the only model that appeared to approach the ECG as a conduction-system problem rather than primarily a morphology problem.
It recognized severe bradycardia. It recognized that the atrial and ventricular rates were different. It recognized that the relationship between P waves and QRS complexes was abnormal.
Its final diagnosis was still wrong, classifying the tracing as complete heart block rather than second-degree AV block with 2:1 conduction. But it was the only model that arrived in the correct neighborhood.
What Did We Learn?
The main takeaway wasn’t that the models missed the diagnosis, but how they did so.
Most systems discussed morphology well: ST segments, T waves, axis, repolarization, bundle branch blocks, and ischemic patterns with clinically plausible language.
Several systems generated detailed differentials, cited literature, and referenced advanced concepts like modified Sgarbossa criteria, yet most struggled with the essential task in this case. Count the P waves. Count the QRS complexes. Recognize that every other atrial impulse fails to conduct.
Except for Gemini, every interpreting model missed the AV conduction issue.
A Reality Check
At this point, it would be easy to conclude that AI simply can’t read ECGs. After all, every system that attempted interpretation missed the correct diagnosis, and some missed it by a wide margin.
After running these tests, I uploaded the same ECG to ECG-GPT, an experimental ECG-specific model developed by the Cardiology AI Research Laboratory. Its interpretation was:
Sinus rhythm with second-degree atrioventricular block with 2:1 atrioventricular conduction. Left bundle branch block. Abnormal ecg
That’s essentially the correct answer. More importantly, it changes how we should think about the remaining results.
The problem isn’t that AI can’t read ECGs. The problem is that most of the systems I tested aren’t actually ECG interpreters. OpenEvidence, Doximity Ask, Vera Health, Claude, ChatGPT for Clinicians, and Gemini were all built for broader purposes. Some are clinical search tools. Some are clinical assistants. Some are frontier language models with image capabilities. None were designed primarily as dedicated ECG interpretation systems.
When physicians upload an ECG into a medical chatbot, they may assume they’re using an AI ECG reader. In reality, they are likely using a clinical assistant that happens to accept image uploads. Those aren’t the same thing, and based on this experiment, the difference may matter more than most of us realize.
The Bigger Problem
There’s another lesson here that extends beyond ECGs. None of the systems that attempted interpretation told me beforehand that they might struggle with this particular task. None explained whether they had been trained or evaluated on ECG interpretation. Instead, I had to discover their limitations experimentally.
That should make clinicians uncomfortable. We’re increasingly being asked to incorporate AI into clinical workflows, yet we’re often given very little information about how these systems perform and whether they have been evaluated at all. The burden of discovering those limitations falls on the clinician using the tool, which is not appropriate.
In this case, the limitations were relatively easy to identify because I already knew the correct answer. That’s not always true in clinical practice.
Final Grades
These grades reflect overall performance on this specific ECG. Systems that appropriately declined interpretation were not penalized for refusing to perform a task outside their stated capabilities.
A: Heidi Health, Glass Health
Declined interpretation rather than providing an unreliable answer.
B: Google Gemini
The only model that recognized the tracing as an atrioventricular conduction disorder. Misclassified the ECG as complete heart block rather than second-degree AV block with 2:1 conduction.
C+: Claude
Correctly identified a normal axis and recognized organized atrial activity, but missed the conduction abnormality that defined the case.
C: ChatGPT for Clinicians
Correctly identified the left bundle branch block but missed the AV block and overcalled acute coronary occlusion.
C-: Doximity Ask
Recognized organized atrial activity but missed the AV block, ventricular bradycardia, and left bundle branch block.
D: Vera Health
Focused on ischemic differentials while missing the underlying conduction abnormality.
F: OpenEvidence
Interpreted the tracing as atrial fibrillation with possible STEMI, effectively describing a different ECG.
Bottom Line
The surprising result wasn’t that the models missed the diagnosis. It was that the two highest grades went to systems that chose not to answer.
Among the systems that attempted interpretation, Gemini came closest because it recognized that the tracing represented an atrioventricular conduction disorder. ECG-GPT demonstrated that AI can, in fact, correctly interpret this ECG when the model is specifically designed for the task.
The question isn’t whether AI can read ECGs. The question is whether the AI you’re using was actually built to do so.
This is a great example of why AI should support, not replace, clinical reasoning. An important point here is that a tool may sound confident and clinically fluent while still missing the basic task in front of it. That’s why clinician knowledge still matters so much. AI can be helpful, but clinicians need the foundation to know when the output makes sense, when it doesn’t, and when the tool isn’t appropriate for the task.